
Pregnancy and childbirth complications have led many women of childbearing age in developing countries to their early graves.
According to the World Bank, over 99 per cent of recorded maternal deaths occur in developing countries.
Maternal mortality is defined as the death of a woman during pregnancy, childbirth or within a year after the end of a pregnancy.
Data from the World Health Organisation revealed that about 287,000 women died during pregnancy and after childbirth in 2020. Out of these figures, Sub-Saharan Africa accounted for around 70 per cent of maternal deaths.
The major contributors to maternal deaths are; severe bleeding (haemorrhage), infections, high blood pressure during pregnancy, complications from delivery and unsafe abortion.
These contributors are, however, subsets of contributory factors such as unskilled birth attendants, poor referral services, lack of equipped and inadequate hospitals and health providers, poverty and ignorance, among others.
An e-medicine platform, Medscape.com, stated that postpartum haemorrhage (excessive bleeding in a woman who just delivered a baby) was the leading cause of maternal mortality. It accounted for 140,000 maternal deaths per year, indicating that one woman, every four minutes, dies of PPH.
However, bleeding during pregnancy, according to Mayo Clinic, is caused by an incompetent cervix, miscarriage, placenta abruption, preterm labour and uterine rupture, among others.
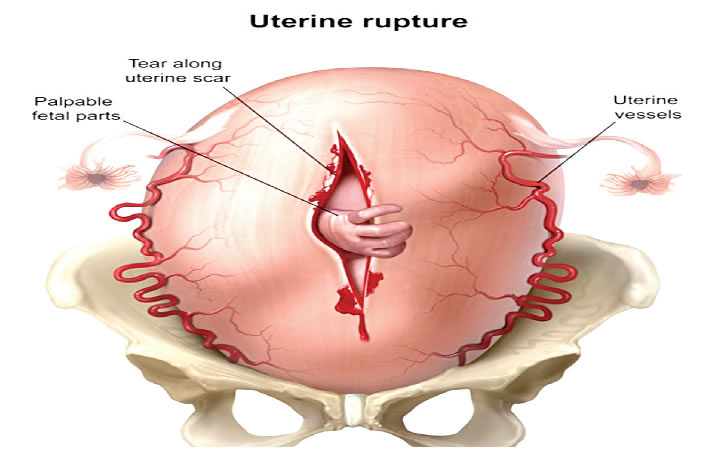
Uterine rupture is the tear of the uterine wall or womb during pregnancy or delivery. It is linked to “fetal distress or maternal haemorrhage” and requires a caesarean delivery.
In another vein, uterine rupture leads to neonatal death, massive bleeding (haemorrhage), hysterectomy (uterus removal), uterus repair, inability to conceive, and complications to the baby, consequently, increasing the risk of maternal mortality.
Previous studies stated that uterine rupture contributed little to maternal mortality but recent studies and observations from Obstetricians and Gynaecologists confirmed an increase in these cases.
A study by S. J. Etuk et al, published in 2019 in biomedical literature, PubMed and titled, ‘Maternal near-miss and death among women with rupture of the gravid uterus: a secondary analysis of the Nigeria Near-miss and Maternal Death Survey’ revealed that in the reviewed year, there were 91,724 live births.
Of this figure, 3,285 women had cases of severe maternal outcomes, and 392 women had uterine ruptures.
It further stated that uterine rupture accounted for 11.9, 13.3 and 8.7 per cent of the severe maternal outcome, maternal near-miss and maternal deaths, respectively.
Late hospital presentation, lack of insurance to cover life-saving interventions and medical personnel problems were avoidable factors that contributed to the death of these women.
The study concluded that uterine rupture contributed significantly to maternal death in Nigeria.
Another study by G.O. Akaba et al in 2013 on ‘Uterine rupture: Trends and feto-maternal outcome in a Nigerian teaching hospital’ revealed that between 2006 and 2010, 82 cases of ruptured uterus were recorded out of the 9,604 deliveries in the hospital.
The researchers stated that the injudicious use of oxytocin (38.7 per cent), previous caesarean scar (28.0 per cent) and prolonged obstructed labour (18.7 per cent) were the causes of the rupture.
A previous study done in 2003 by T. Ogunowo et al, ‘Uterine rupture: UCH, Ibadan experience’ reported 35 cases of uterine rupture out of 4,531 live births. The study carried out between 1996 and 2000 revealed an increase in the cases from 10 years ago.
All the studies from 1996-2000, 2006-2010 and 2019 revealed a percentage increase from 0.72, 0.85 and 11.9 per cent, respectively.
Reacting to the recent increase, the Secretary of the Society of Gynaecology and Obstetrics, Dr Chris Aimakhu, stated that pregnant women at risk of uterine rupture were those who had previous surgery, like CS, myomectomy (fibroid surgery) and abortion; those who had many children, induced labour with oxytocin (a medication that stimulates labour) in previous deliveries, twin deliveries and assisted birth or instrumental delivery.
He explained that those previous processes could cause the uterine wall to be “weak and when the woman goes into an unsupervised labour and contracts, there would be a tear.”
Aimahku noted, “The increase for us now is observational. We are seeing it more often now than last year or two years ago. In the last month, we have seen five to six cases of uterine rupture in the University College Hospital, Ibadan, Oyo State.”
Another public health physician and founder of Quinta Health, Dr Babatunde Adewunmi, stated that last week, there were four cases of uterine rupture at the Federal Medical Centre, Abeokuta, Ogun State.
Mockery of women who have had CS and tried out vaginal delivery, illiteracy and inadequate health education of unskilled delivery attendants, among others, were factors fuelling the rise in uterine rupture.
Commenting on the issue, a Consultant Obstetrician/Gynaecologist at the Department of Obstetrics and Gynaecology, Federal Medical Centre, Yenagoa, Bayelsa State, Dr Ebiye Tekenah, stated that women with a history of caesarean section or surgical procedures, attempting vaginal birth in subsequent deliveries were at risk of uterine rupture.
Tekenah said, “There are various causes but it is common among women who have had a previous caesarean section. This means the uterus has a scar and is at risk of uterine rupture. Pregnant women who do not have a scar but deliver in places with unskilled birth attendants are also at risk of uterine rupture.”
The consultant further stated that the injudicious administration of contraction-improving medications could cause the uterus to over-contract and increase the risk of women who had multiple births when administered.
She explained that the recent increase was caused by the ignorance of women who had CS previously but visited unskilled birth centres in an attempt to have a vaginal birth.
Tekenah added, “It is a common practice in our locality when pregnant women go for an abdominal massage to turn the baby. Even without a scar, this is wrong because the risk of rupture triples when there is a scar and in the process, they cause a tear in the womb. This causes an increased risk of morbidity and mortality. Many times, the baby dies and the mortality rate is as much as 30-40 per cent. If the woman is not taken to the hospital in time, she haemorrhages and dies.”
She urged women with a history of CS to register subsequent births and deliveries in a secondary or tertiary-level health facility, refrain from abdominal massage and attend antenatal clinics regularly.
The doctor further called for an improved family planning service, referral services and transportation, especially in rural areas without well-equipped facilities, to reduce the risk of prenatal and maternal mortality.
On the most common presentation of pregnant mothers suffering uterine rupture, Aimakhu stated, “If it is a complete rupture, the baby comes out of the womb through the tear into the abdominal cavity and you can feel the baby freely in the tummy. Also, there can be bleeding from the vagina or internal bleeding, in which case she is bleeding into the abdomen and then begins to have low blood pressure, rapid pulse and fainting.”
He added, “Another reason for the upsurge is that people use oxytocin which is indicative for stimulating labour but must be administered to patients who do not have a previous scar, are well monitored and given appropriate dosage. Some women past their due date buy an over-the-counter drug called misoprostol and overuse them to induce labour.”
The SOG secretary urged pregnant mothers with the risk factors to attend antenatal and book their deliveries in a facility equipped to handle emergencies.
On his part, Adewunmi stated that although women who have had CS could have vaginal birth deliveries, such deliveries had to be taken in a facility where CS can be done immediately.
He added, “If there is no service for caesarean section, during the trial for labour, a uterine rupture could occur. Some women go to a faith home or traditional birth attendants who give them uterus-contracting medications that can lead to rupture. The uterus is a highly vascularised organ linked to a major artery close to the heart. Therefore, any problem to the uterus or cervix would lead to bleeding.”
The doctor added that pregnant mothers who suffered a fall or hit to their stomach and underwent abdominal massage were further prone to uterine rupture.
Adewunmi said, “Those with congenital defects, for example, those who have a double or malformed uterus, are also at risk of uterine rupture. Also, mothers who have a lot of amniotic fluid will lead to an expansion of the uterus that cause a burst.”
The physician called for “safe motherhood.”
“This involves clean and safe delivery that ensures skilled birth attendants attend to pregnant mothers. Also, women should be educated on the need to attend registered and equipped hospitals for antenatal and child delivery. The government should ensure that most hospitals have trained staff for deliveries,” he added.


{kind=link}